

Part 1: The challenge of defining Long Covid and its prevalence.
Part 1: The challenge of defining Long Covid and its prevalence.
Long Covid Summary Series: What are the odds of getting Long Covid (adults and children) after SARS-CoV-2 infection, and who is most at risk?

I will be summarizing much of the research gathered around Long COVID over the last few years. This is part 1 of this series.
Defining Long COVID remains complex
Long COVID, also known as post-acute sequelae of SARS-CoV-2 infection (PASC), gained notoriety during the COVID-19 pandemic for its wide range of symptoms across multiple organ systems, some characterized as just subtly bothersome to others more severe, long-lasting and debilitating. Long COVID (LC) are continuing, relapsing, or newly onset post-COVID conditions or symptoms that persist for four or more weeks after an acute infection.

Defining long COVID has remained challenging, but there is still consensus that it affects multiple bodily systems, including the immune, respiratory, cardiovascular, gastrointestinal, neuropsychiatric, reproductive, and musculoskeletal, among others. Long COVID is varied in its symptomatology, and thus likely results from different underlying pathophysiological mechanisms (to explore in Part 2).
Estimates on the incidence (# of new people that get the condition) and prevalence (# of people with the condition in the community, including new cases) of Long Covid vary widely across different studies, likely because of the differences in methods and inclusion criteria. The vast variability in reporting, definitions, and heterogeneity in the population, along with the overall lack of consensus on what constitutes long COVID and the wide range of reported symptoms have made it challenging to compare data. Furthermore, symptoms of pandemic fatigue, as well as the inconsistent, variable, and relapsing nature of long COVID obscure the evaluation of symptoms.
The vast variability in reporting, definitions, and heterogeneity in the population, along with the overall lack of consensus on what constitutes long COVID and the wide range of reported symptoms have made it challenging to compare data.
Regardless of the differences in estimates across different studies, the overall prevalence amongst those who have had COVID-19 has declined in the last couple of years, with a subtle increase observed at the beginning of the current year.
According to the U.S. Census Bureau and National Center for Health Statistics Household Pulse Survey, nearly 18% of adults in the U.S. have experienced long COVID, and nearly 7% are currently experiencing it (data from March 5 to April 1).
The most common symptoms, as reported by the CDC are:
Fatigue
Shortness of breath
Cough
Joint pain
Chest pain
Brain fog (difficulty thinking clearly and focusing)
Depression
Muscle pain
Headache
Fever (may come and go)
Heart palpitations (feeling of the heart pounding)
Who is at the highest risk for Long Covid?
Risk factors have been identified.
While anyone infected can be susceptible to Long COVID, it has been found to occur more frequently in people who have had severe COVID-19 illness, also making the correlation stronger across older individuals.
Women are disproportionately prone to experiencing persistent Long COVID/PASC symptoms, including fatigue, cognitive impairment, respiratory issues, and musculoskeletal discomfort, even after recovering from acute COVID-19.
Other risk factors have also been identified. A longitudinal investigation of 309 COVID-19 patients from initial diagnosis to convalescence (2-3 months later), identified four risk factors at the time of initial COVID-19 diagnosis:
Higher viral loads at time of infection
Type 2 diabetes
Epstein-Barr virus reactivation
Specific autoantibodies
Having specific immunoglobulin signatures (decreased IgM & IgG3), a history of asthma and symptomatic primary COVID-19 infection have also been identified as risk factors.
The NIH-funded RECOVER trial, including over 250 participants both infected and uninfected with SARS-CoV-2, found significant immune cell differences in those with Long COVID. Long COVID patients had higher levels of non-conventional monocytes and activated B lymphocytes, and lower levels of type 1 dendritic cells and central memory T cells. Stronger antibody responses to the SARS-CoV-2 spike protein and Epstein-Barr virus were also observed. Machine learning identified low cortisol levels as the strongest predictor of Long COVID, alongside elevated galectin-1, high antibodies against EBV, and reduced immune cells.
A prospective study following 106 COVID-19 patients and 68 non-COVID-19 controls for 6 months analyzed 258 fecal samples and found a correlation between the gut microbiota’s initial composition and diversity, and the development and persistence of long COVID symptoms, indicating that the gut microbiome could potentially serve as a biomarker for predicting PACS and might be a target for therapeutic interventions.
What are the odds?
The true prevalence, and hence risk of long COVID has remained challenging to quantify due to several factors. First, it encompasses a large range of symptoms, from fatigue and brain fog to respiratory issues and organ damage. The diversity and variability of symptoms make it difficult to identify and quantify, and many individuals impacted may not seek medical attention. That aside, their symptoms may not even be recognized as LC by healthcare professionals.
Data collection on long COVID is subject to confounders such as self-reporting, recall bias, and the absence of standardized assessment tools. Tracking these symptoms over time and distinguishing them from other chronic conditions requires longitudinal studies and robust data collection methods. Studies may use different criteria for defining long COVID, as well as include different populations, such as hospitalized patients, healthcare workers, or the general public, which can affect the reported incidence of long COVID.
Studies may also have variability in follow-up time. Long COVID is characterized by symptoms persisting for weeks or months after the acute phase of an infection. Because some symptoms may resolve, this may lead to differences in estimates of prevalence. It has been proposed that post-COVID syndrome could be classified as either acute or chronic, depending on whether symptoms last beyond 12 weeks after the initial diagnosis. However, it remains unclear whether chronic post-COVID is an extension of acute post-COVID or an entirely separate condition with its own unique risk profile.
Individual host factors such as age, gender, pre-existing health conditions, attitudes and the severity of the initial COVID-19 infection further conflate interpretation of the data. Estimates of prevalence also depend on the identification of COVID-19 cases, as these constitute the denominator. The accuracy and availability of testing across different settings and time periods, especially during waves, thus will impact the overall figures and risk assessment. Biases from a lack of control arms and confounding variables, as well as limited details on participant recruitment and response rates also impact pooled analyses.
While the WHO has placed prevalence estimates at around 10-20%, 2022 survey data from the U.S. Centers for Disease Control and Prevention show that Americans have experienced long COVID at an estimated rate of nearly 7%. In the UK, 1.9 million or 2.9% of the population were experiencing self-reported long COVID (symptoms continuing for more than four weeks) as of 5 March 2023.
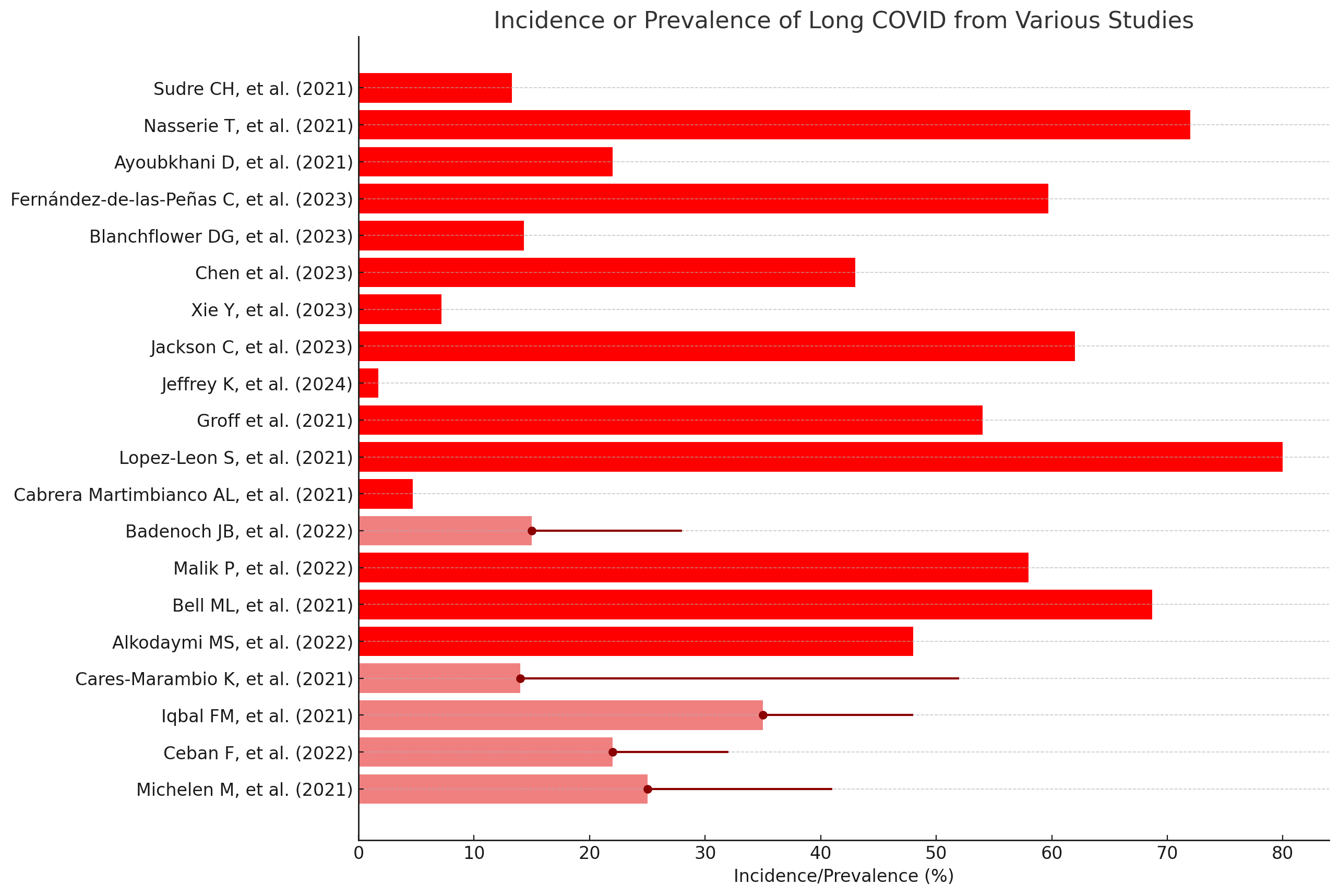
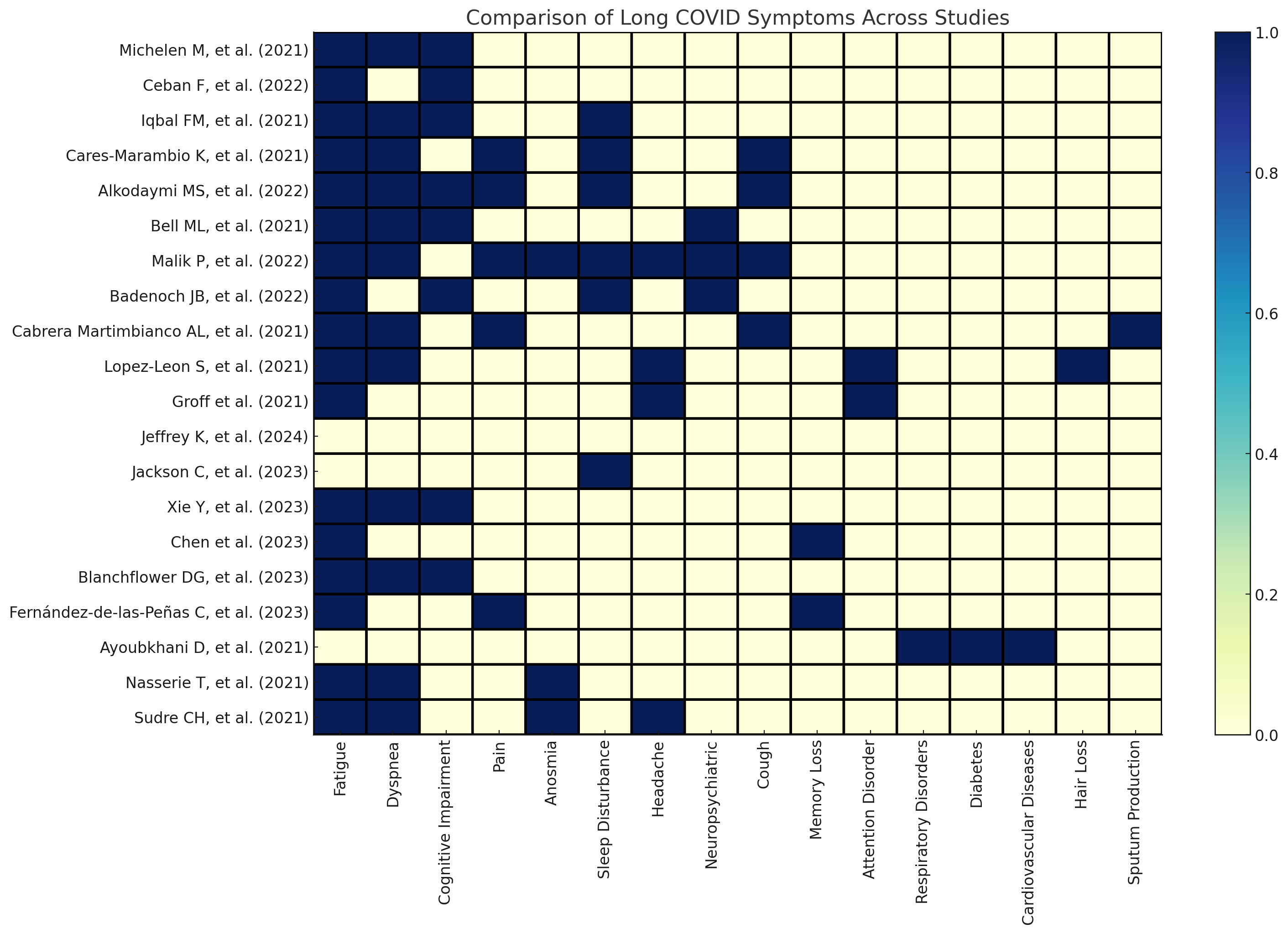
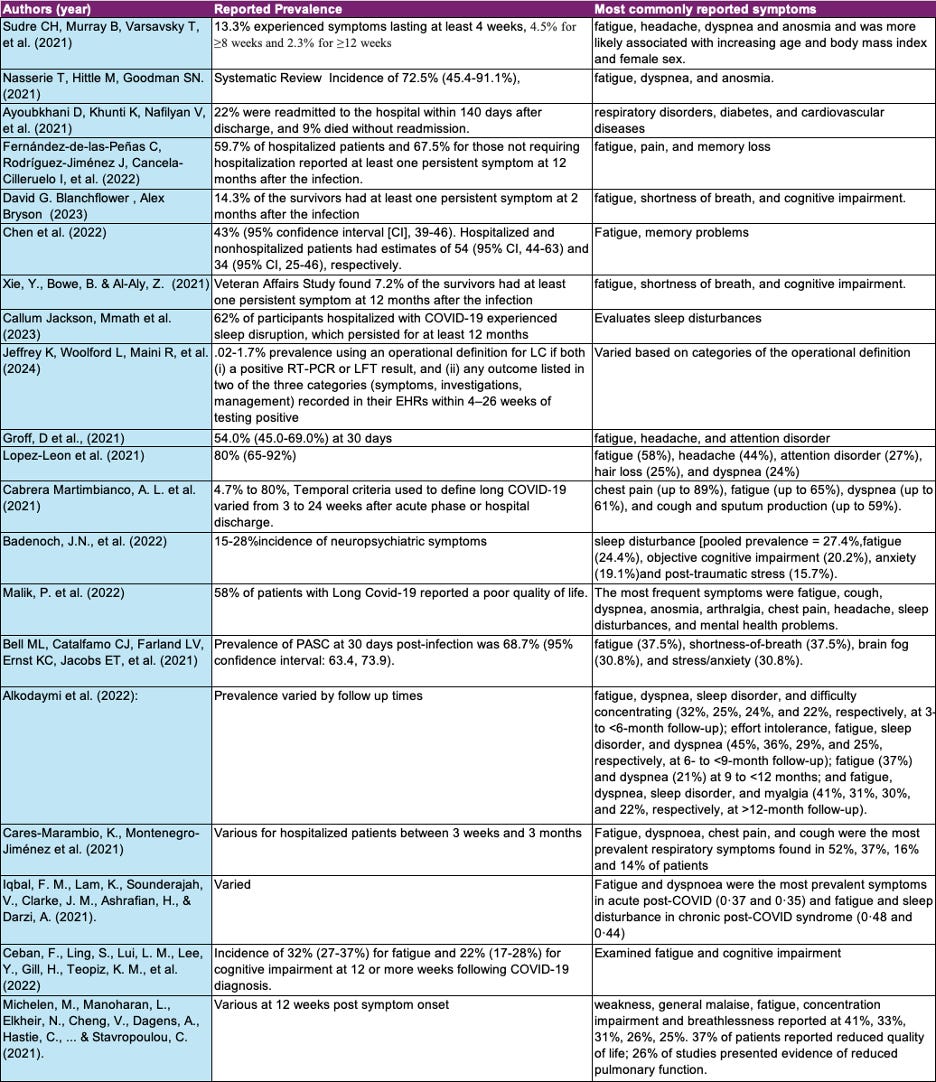
Below, I present a summary of the prevalence or incidence of long COVID along with the most widely reported symptoms across different studies, meta-analyses, and systematic reviews, followed by details for each study in one chart.
Pediatric Population Risks
Children and adolescents exhibit symptoms comparable to those of adults, with the most frequently reported including fatigue, shortness of breath, sleep problems, abdominal pain, dizziness, headaches, memory loss, and difficulty concentrating.

Initial evidence indicating that SARS-CoV-2 infection causes dysregulated immune responses emerged from pediatric cases of multisystem inflammatory syndrome in children (MIS-C). This condition, characterized by widespread organ involvement, shares clinical features with other hyperinflammatory syndromes such as Kawasaki disease, toxic shock syndrome, and macrophage activation syndrome.
Most meta-analyses and systematic reviews have found the prevalence of Long Covid in pediatric patients to be at least over 10%. One meta-analysis across 12,424 individuals found that the overall prevalence of long COVID was 23.36%. The most commonly reported symptoms were generalized (19.57%), respiratory (14.76%), neurologic (13.51%), and psychiatric (12.30%).The prevalence of symptoms decreased over time, with 26.41% affected at 3-6 months and 14.89% after 12 months. Higher prevalence of long COVID was seen in those over ten years old, with multisystem inflammatory syndrome, or severe initial symptoms. Factors such as older age, female gender, poor physical or mental health, chronic condition, severe infection, or having more symptoms increased the likelihood of long COVID in pediatric survivors, as confirmed across several studies.
Another meta-analysis across 80,000 children and teens found the prevalence of Long Covid, as defined by the presence of one or more symptoms more than 4 weeks following a SARS-CoV-2 infection, at 25.24%. For hospitalized patients, the prevalence of long-COVID was 29.19%. The most common symptoms and percentage of prevalence associated were mood symptoms, fatigue, sleep disorders, headache, respiratory symptoms, congestion, cognitive symptoms, exercise intolerance, and altered smell.
One study found that while infected adolescent girls were roughly 4 times more likely to experience Long Covid symptoms than exposed counterparts, moderate or severe persistent symptoms were not statistically more common in infected adolescent boys aged 14–18 or in infected children <14 years. The number of persistent symptoms reported by individuals was associated with the number of persistent symptoms reported by their household members.
The prevalence of Long Covid after infection with the Omicron variant has also been reported on. Across 332 first-positive, 243 reinfected, and 311 test-negative children and young people who filled in the online questionnaires, the proportion of children and young meeting the long COVID research definition at both 3 months and 6 months was 12.1% (first positives), 16.1% (reinfected), and 4.8% (always tested negative).
Notably, infants have been found to account for over a fifth of children <18 years of age hospitalized for severe acute COVID-19, commonly manifesting with respiratory symptoms and complications. During the Omicron period, COVID-19-associated hospitalizations in children aged 0-17 were four times higher than during the peak of the Delta period. The largest increase in hospitalization rates was observed in children aged 0-4 years.
Do Vaccines Help?
Several studies have also found that people who are not vaccinated against COVID-19 and become infected may have a higher risk of developing Long COVID relative to vaccinated individuals. However, the magnitude of vaccines’ protective effect size varies considerably across them. While some studies report a 50-66% reduction in the likelihood of developing some long COVID symptoms compared to unvaccinated counterparts, others report roughly a 10%-45% lower risk of sensory, blood and hematologic, skin and subcutaneous, and non-specific COVID-19-related disorders relative to unvaccinated matched individuals.
The data around whether vaccines may improve long Covid symptoms also exhibits variability. One pre-print found that the rate of complete remission from long COVID symptoms doubled in vaccinated patients relative to unvaccinated long COVID ones. Another survey in the UK among vaccinated long Covid survivors found that 24.6% had symptoms that remained unchanged, 18.7% reported worsening symptoms and 56.7% reported improvement.
Final thoughts
Long COVID, or post-acute sequelae of SARS-CoV-2 infection (PASC), continues to present a complex and multifaceted challenge for researchers and healthcare providers. The condition affects multiple organ systems and manifests in a wide range of symptoms, making it difficult to define and quantify. Studies indicate that a significant portion of COVID-19 survivors experience persistent symptoms, with estimates of prevalence varying widely due to differences in study methods and populations.
The complexity of Long COVID underscores the need for ongoing research to better understand its pathophysiology, risk factors, and effective treatment strategies. As our knowledge evolves, it is crucial to continue monitoring and supporting those affected by this condition, ensuring they receive the care and attention necessary to manage their long-term symptoms.
Stay tuned for Part 2: What causes long COVID and what treatments are there on the horizon? Part 2 will examine the different hypotheses for its pathophysiology and the evidence around each of these, as well as ongoing data from different clinical trials for the treatment of symptoms.