


The Fluoride Fight Was Never About Health
It’s About Undermining Trust in Experts, Eroding Public Health Protections, and Being Oppositional

This week, the administration announced plans to remove concentrated ingestible fluoride prescription drug products for children: think drops or supplements. This is not fluoride in our water, but rather products available to parents to supplement in areas of low water fluoride content, under the guidance of their providers. At the same time, Florida’s Governor, Ron DeSantis, like Utah, has signed a bill to ban fluoride in their water.

So why is this happening?
They claim it’s about “protecting children” from fluoride’s supposed effects on IQ, weight gain, and thyroid function. But if you follow the citations, you’ll find it’s a patchwork of weak associations and overstretched animal studies, not a solid body of evidence. This isn’t science. This is a decoy, a costly one.
More specifically, Marty Makary's announcement references a meta-analysis looking at the effects of fluoride on gut microbiota. Let’s talk about the actual research they are citing.
90% of the studies are from Asia.
88% of the 42 studies they reference are animal studies, not human.
And even the authors admit we don’t know what constitutes a “healthy” microbiome.
The review states:
“Fluoride at low levels (<2 mg/L NaF in humans and <25 mg/L NaF in animals) did not affect gut microbiota. Although effects at high doses are inconsistent, impacts could be seen in overall microbial diversity change, change in relative abundance of specific taxa, and changes in the metabolism of present microbiota. Shifts in any of these aspects... can lead to health implications.”
That last line? It’s speculative. It's the scientific version of "something might happen."
Meanwhile, most of the U.S. population is already well under 1.5 mg/L in water fluoride concentration.
And yet, they are building public health policy around cherry-picked results and speculative mechanisms. Let’s dig even deeper.
Why Many Fluoride Studies are Statistically Thin and Clinically Meaningless
The problem with fluoride studies is that they are vastly weak and inconsistent throughout. When effect sizes (how well something works or causes harm) are patchy across data sets, it points to either weak effects that are clinically meaningless or confounding variables (or both). I have discussed this before with Dr. Jess Steier. Most recently, we reviewed a meta-analysis looking at the association between fluoride and IQ. A meta-analysis sounds compelling, but it ignores one basic rule of data science: GIGO, or Garbage In, Garbage out.
A meta-analysis is only as strong as the studies it includes. In this case, many of the underlying studies are methodologically weak, making the overall conclusions unreliable, especially for informing U.S. policy.
Key Problems:
Cross-sectional design: Most studies were snapshots in time and cannot show cause and effect.
Small sample sizes: Many involved fewer than 300 children, making the findings statistically fragile.
Poor control of confounders: Factors like socioeconomic status, parental education, and exposure to other neurotoxins were often ignored.
Statistical errors: Some studies misused basic statistical methods (e.g., using a paired t-test on independent groups).
Inconsistent or flawed dose-response patterns: Some studies showed effects only in narrow exposure windows, contradicting basic toxicological principles.
Questionable exposure measurement: Many relied on urinary fluoride, which reflects short-term intake and is influenced by hydration, not a reliable marker for long-term exposure.
Here as some of the studies included here (for a longer list, refer to our Substack):
Yu (2018) showed effects only in a narrow fluoride range, with no dose-response consistency.
Cui (2020) actually found no significant effect, though often misrepresented.
Rocha-Amador (2007) had strong design but couldn't isolate fluoride from arsenic exposure.
Seraj (2012) controlled for iodine but showed no clear dose-response.
Poureslami (2011) and Eswar (2011) reported small or no differences, and this is often completely ignored.
Some of the more common themes across these studies:
Many studies were conducted in areas with very high natural fluoride, not fluoridated water. This can skew a trend, making it seem like something is more likely to occur across a homogeneous population, whereas it is likely happening in specific sub-populations.
IQ differences reported were small, often within the margin of error for IQ tests.
Environmental factors and co-exposures were often ignored, especially in regions with high industrial pollution.
Take another widely-cited study. It found that maternal fluoride exposure increased IQ in girls but decreased it in boys. But that’s not how neurotoxins work. How could you see an effect in boys but not in girls? I will tell you how: data parsing or improper binning, as I discussed in the post below.

The study failed to control for exposure in children post-birth as well, meaning that the fluoride consumption was not accurately tabulated even. They also included children with IQs near 70 in their analysis, extreme outliers that dramatically skew averages. An IQ of 70–75 signals possible intellectual disability and must be interpreted in clinical context, not dumped into a group average to make the numbers look dramatic.
Another study from China claimed fluoride exposure was associated with a 0.13–0.18 increase in BMI Z-score. Statistically significant? Sure. Clinically relevant? Absolutely not. That’s ~1/8th to 1/6th of a standard deviation, i.e., a tiny blip well within normal variation. That is like arguing that because there was a 1-3% variation in weight (well within normal in a population), we should blame the water.
It gets weirder. That same study found that fluoride was linked to increased height: a 0.129 unit increase in height z-score. So... fluoride makes you taller and heavier? That doesn’t suggest a toxic effect. That suggests noise. Or confounding. But not causation.
Notably, the effects were stronger in girls and in children whose fathers had lower education levels, classic signs of underlying socioeconomic disparities, not fluoride exposure.
This means that the findings cited to argue that fluoride reduces IQ or increase BMI are based largely on low-quality, poorly controlled, and geographically limited studies. Most show tiny differences, with little clinical relevance, and cannot prove causation.
For public health policy, especially in countries like the U.S. with regulated fluoride levels, these studies provide no solid basis for reversing or questioning community water fluoridation. And yet, this is the “evidence” they’re using to dismantle a foundational public health measure.
But What About the Gut Microbiome?
Not surprisingly, the newest fear lever is the microbiome. The logic goes:
“If fluoride impacts bacteria in the mouth, maybe it harms the gut, too.”
Except… it doesn’t. The evidence available doesn’t even show that.
First, again, most of the cited data is from animal studies. Many used absurdly high doses. For instance, in one study cited, rats were given water with 100 mg/L NaF.
Let’s put that in context:
A 1 lb rat drinks about 10 mL per 100 g of body weight per day, so at 100 mg/L, that's ~10 mg/kg/day of fluoride. Adjusting for body surface area (correction factor of 0.162) to a human equivalent dose: ~1.62 mg/kg/day.
Our drinking water has fluoride levels around 0.7–1.0 mg/L, and the average child consumes about 1-2 mg/day, or 0.03-0.06 mg/kg/day. That’s 30–50 times lower than what was used in the rat models.

Meanwhile, the human studies using both low (1–2 mg/L) and high (10–15 mg/L) fluoride in that very same meta-analysis found no significant effect on short-chain fatty acids (SCFAs), a key marker of microbial function. What does this mean? Likely, there aren’t meaningful effects to our gut microbiota that translate to adverse health outcomes.
The gut microbiome is incredibly complex, and yes, it plays a role in many aspects of health. But it has also become a catch-all explanation for everything we don’t fully understand yet.
When people say, “It affects the gut microbiome!” as a reason to panic, what they often mean is: “We found something changed (typically in rodents who were exposed to something on mass), and we don’t know what it means, but it could be bad!”
Not all changes are bad, and not all changes are meaningful. This is a classic conflation of statistical effect with effect size. It is also a false balance between what “could be,” rooted in weak studies, and “what is” from robust data. Just because anything could be possible doesn’t mean everything is equally likely or important.

Also important: fluoride’s primary mechanism of action isn’t as an antimicrobial.
It stabilizes tooth enamel by bonding with hydroxyapatite and converting it into fluorapatite (you also get fluorohydroxyaptite), making teeth more resistant to acid and decay.
Here is a really great, simplified explanation. Tooth enamel is mostly made of a mineral called hydroxyapatite, which contains calcium and phosphate. Normally, there’s a balance between these minerals in your saliva and your teeth. But when the pH in your mouth drops below 5.5, like after eating or drinking acidic foods, it starts to break down enamel in a process called demineralization.
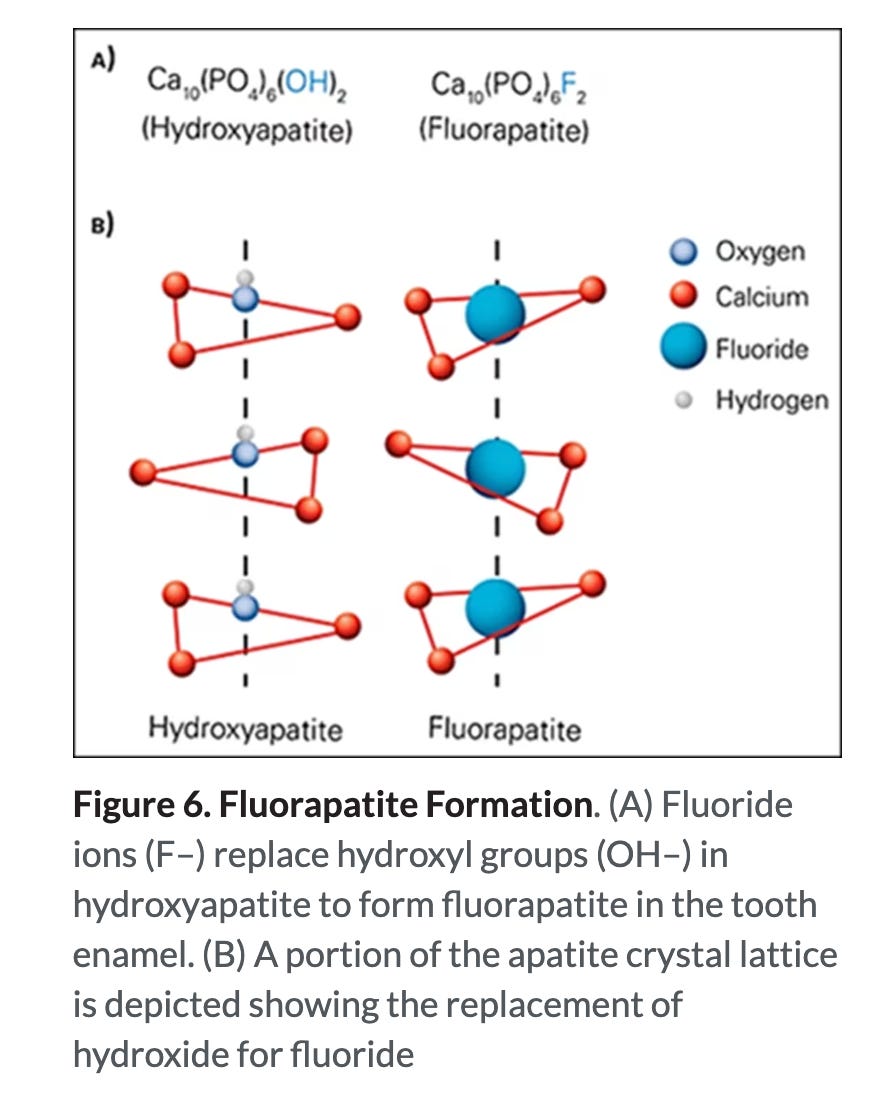
While topical fluoride (like your toothpaste or fluoride varnishes) directly protects teeth, water fluoridation creates more chronic exposure. When we ingest it, it then recirculates in our saliva. When fluoride is present, it helps form a stronger mineral called fluorapatite instead of regular hydroxyapatite during remineralization.
Fluoride replaces hydroxyl (OH) groups in the tooth’s crystal structure (in hydroxyapatite), making the enamel stronger and more resistant to acid. Fluorapatite doesn’t dissolve as easily, so teeth become stronger and less likely to decay, even in acidic conditions.
How do we know Fluoride Works?
There are multiple lines of evidence for the effectiveness of fluoride.
From a Cochrane systematic review we know that community water fluoridation reduces tooth decay by 35% in baby teeth and 26% in permanent teeth compared to non-fluoridated areas, and that the effect is strongest when fluoride is introduced before age 5. The same review states that it found insufficient information about the effects of stopping water fluoridation. However, that is where real-world data fills in the gap.
One of the better way of looking at causal effects are dose-response studies, whether intentionally planned or as part of circumstantial experiments in real life.
We know that removing fluoride from community water, as they did in Juneau, AK, resulted in a significant increase in cavities and children and increased dental costs. In that area, the rate of tooth decay in young children rose significantly, from 14.4% to 30.3% over time, even though Juneau residents generally have higher socioeconomic status, which is typically linked to better dental health.
This follows the trend observed in Calgary as well, where fluoride was removed in 2011. Guess what happened? A decade later, voters there voted to put fluoride back into the water (yes, due to increased cavities). The effort is delayed by supply chain bottlenecks. Yes, even four years later. It is not inexpensive either. The infrastructure costs to reintroduce fluoride at Calgary’s two water treatment plants are $28.1M. That wasn’t even the worst part. The number of prescriptions for IV antibiotics in Alberta’s Children’s Hospital grew by 700 percent, indicative of more systemic infection, not just limited to teeth.
But fluoride isn’t naturally made in the body…!
Many beneficial substances aren’t naturally made by the body either.
Vitamin C isn't synthesized in the human body; we get it from food.
Iodine, zinc, and fluoride are all trace elements we get externally, yet they play roles in health.
Fluoride isn’t essential for life, but it is beneficial for dental health when delivered appropriately.
Fluoride exists in natural water sources at varying levels depending on local geology. Trace amounts of fluoride are also found in bones and teeth, even without fluoridated water, because we absorb it from the environment and diet. Lastly, natural doesn’t make a substance inherently worse or better either. "Natural" says nothing about safety. Dose and context are what matter. Arsenic, mercury, and lead are natural and toxic. Botox is one of the most deadly toxins known to humans, yet medically used in controlled doses.
What about Europe? What about it?
Some point to Europe, arguing they don’t fluoridate their water. This, we discussed at length as well. In Europe, fluoride is delivered in different routes to ensure widespread access. While over 13 million people receive fluoridated water, more than 70 million benefit from fluoridated salt in countries like Germany, France, and Switzerland. Other approaches include school-based fluoride programs, milk fluoridation, and natural water sources with optimal fluoride levels. Europe also has universal public dental coverage that includes regular fluoride treatments. Much of the population in the U.S. can barely get health care here.

What They Really Want
Let me be clear, this isn’t about gut health or fluoride being bad (it isn’t).
The attacks on fluoride are part of a broader strategy. It’s about being oppositional and further eroding trust in experts and public health.
If you can convince people that fluoride is dangerous, despite a mountain of evidence to the contrary, you’ve set the stage to undermine vaccines, demonize public health agencies, and erode the credibility of scientists altogether.
They frame it as “parental rights,” but it’s about dismantling shared responsibility. They want to shift the burden to individual families—
“Avoid sugar. Just brush better.”
That ignores real structural issues: socioeconomic disparities, unequal access to dental care, and genetic predispositions that make some people more vulnerable to tooth decay.
And if you don’t understand the subtext, let me spell it out:
If illness is framed as a personal failure, then society doesn’t owe you programs to help you. No public policy. No safety net. No infrastructure.
You’re just a bad parent. Or a lazy one.
Science Is the Target
Attacking fluoride is just the beginning. They’ve already gone after vaccines. They’ve smeared scientists like Dr. Fauci. The goal is to reject expertise and sow distrust.
Public health measures like water fluoridation are some of the most successful interventions in history. Better dental health is linked to lower risks of heart disease and even dementia.
Undoing that doesn’t make us safer. It makes us sicker, more vulnerable, and less able to fight back. And when that happens, people will look for someone to blame. But hey, maybe that’s exactly the point.